Here's a surprising fact about homocysteine: the best supplements for lowering it are cheap B vitamins you can buy anywhere. Most people waste money on expensive heart health formulas. But decades of research point to a few simple nutrients instead.
Homocysteine is a blood marker tied to heart disease and cognitive decline. When it's elevated, it usually means your body is short on B vitamins. Correcting that shortage brings levels down fast — often within weeks. The payoff: better cardiovascular markers and protection against nerve damage and anemia.
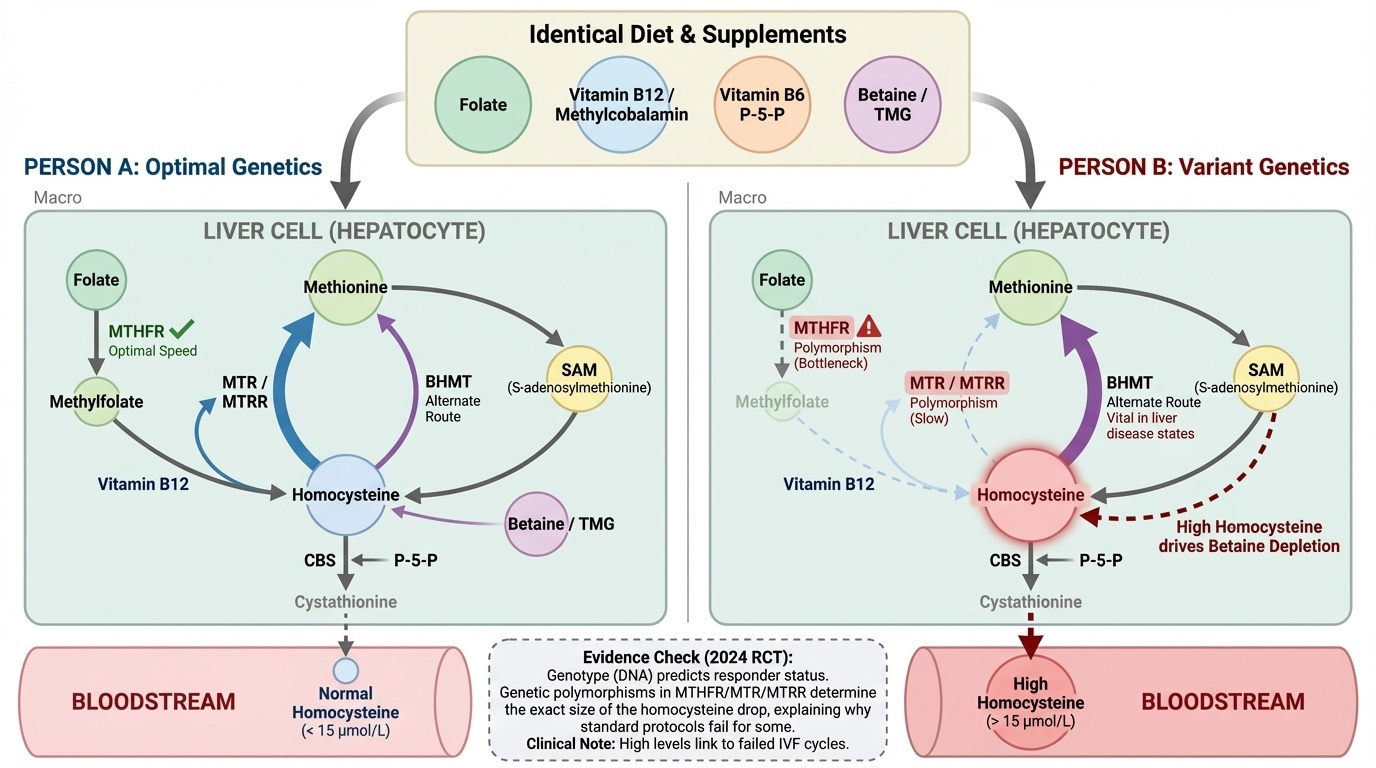
Here's exactly what to take. Start with 400–800 mcg of folic acid daily — this alone cuts homocysteine by about 25%. Add 500–1,000 mcg of vitamin B12 daily for an extra 7% drop. If levels stay high, add 25–50 mg of vitamin B6 daily. For stubborn cases, betaine (trimethylglycine) at 3–6 grams per day works through a completely different pathway. Get your levels tested before you start, and retest in 2–3 months.