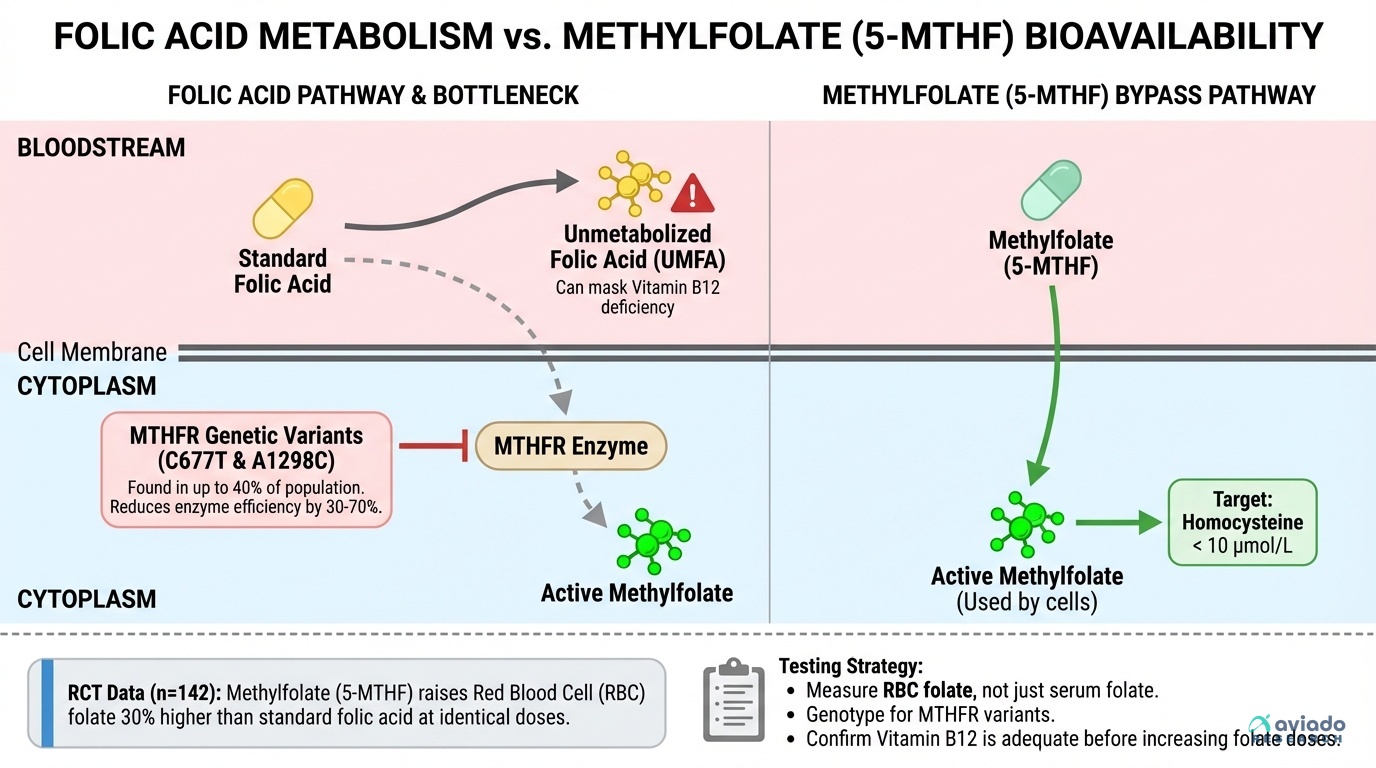
A surprising number of people take folic acid and get little benefit. Your body must change folic acid into methylfolate. Many people do this slowly because of MTHFR gene variants.
This means you may look “fine” on simple tests, yet still run low in cells. If you have an MTHFR variant, folic acid can leave more unmetabolized folic acid in your blood. You can avoid this by using methylfolate instead.
Take 400–800 mcg of 5-MTHF daily for most goals. Recheck RBC folate in 12 weeks, not just serum folate. Also check homocysteine; aim for under 10 μmol/L. Confirm vitamin B12 is adequate before higher folate doses.