Here's the surprising truth about vitamin E: it only works if you're actually deficient. Decades of research seemed to contradict itself—until scientists realized almost nobody was checking vitamin E status before testing supplements. If your levels are already normal, taking more won't do much. But if you're running low, the difference is dramatic.
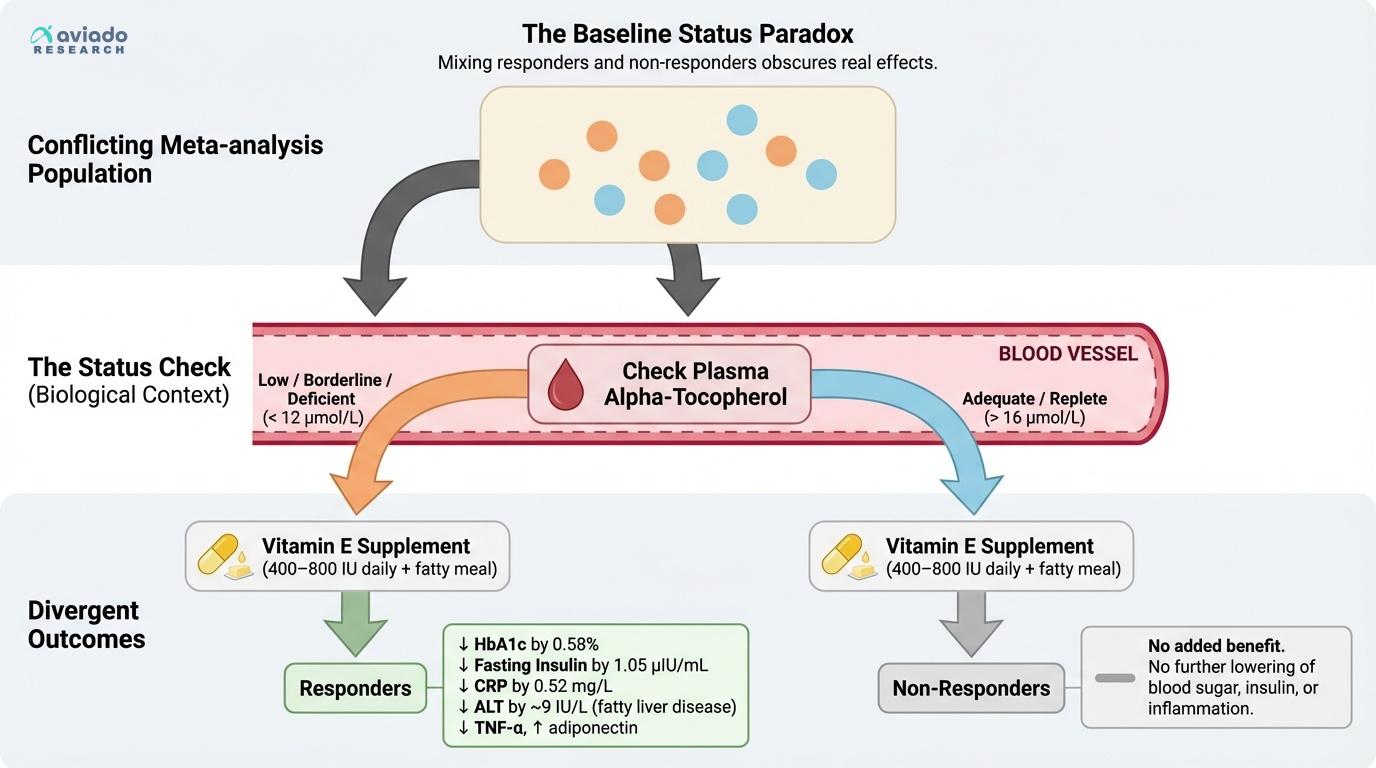
This matters because most people assume more antioxidants are always better. Two major studies looking at blood sugar control came to opposite conclusions. The catch? Studies finding real benefit only included people who were deficient in vitamin E. Studies showing no effect included everyone, regardless of their baseline status. This baseline paradox explains why your results may not match what you read online.
If your blood test shows low plasma alpha-tocopherol, vitamin E can cut your HbA1c by 0.58% and drop your fasting insulin by 1.05 µIU/mL. The effective dose is 400 to 800 IU per day, taken with a fatty meal for best absorption. But if your vitamin E level is already normal, extra supplementation likely won't help. The bottom line: check your vitamin E status first.