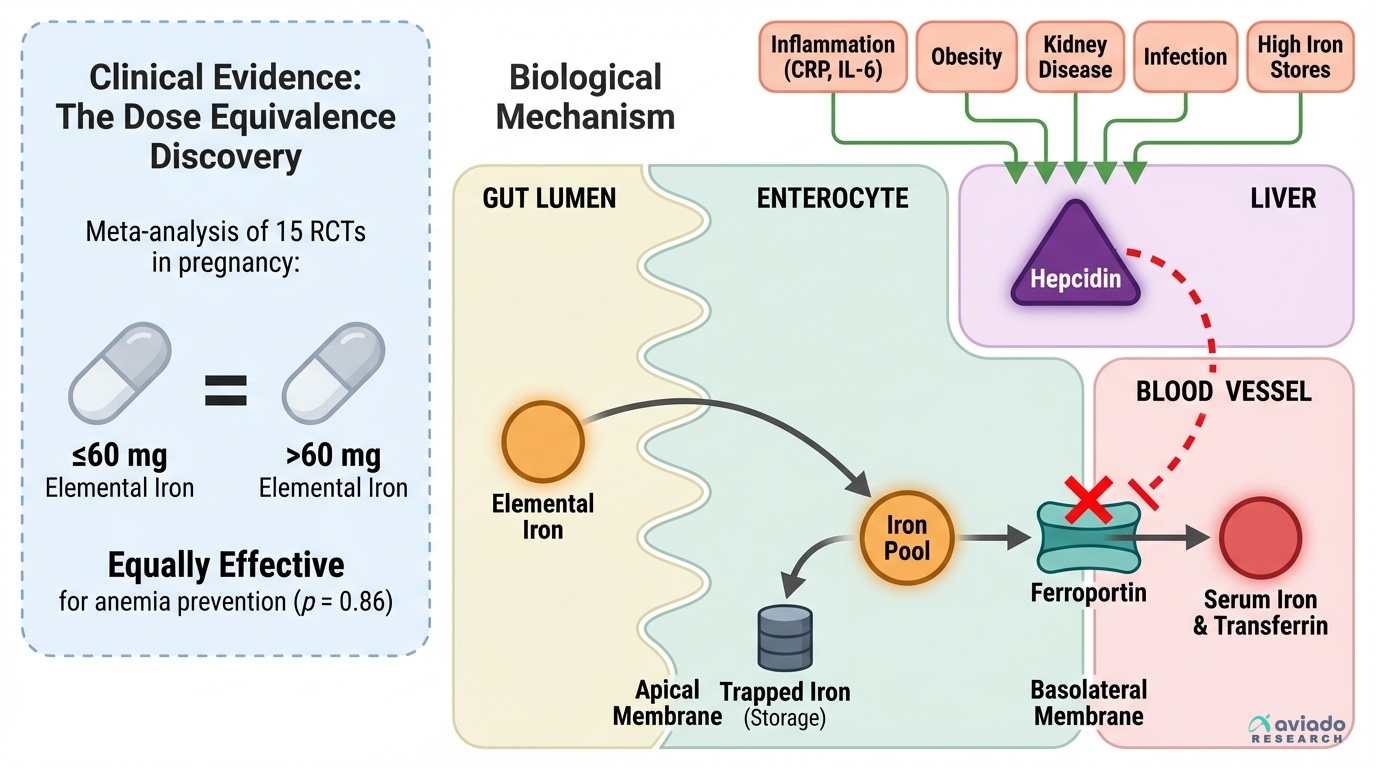
A surprising finding shows iron dose is not the main issue. Many people take 100–200 mg daily. They think more iron works better. But trials in pregnancy found ≤60 mg works the same.
This means you should not chase bigger doses. Your body may block iron first. A hormone called hepcidin can shut the iron “gate.” If your hepcidin is high, you absorb little iron. Then even high doses may not help you.
Start with 60 mg elemental iron once daily. Recheck labs in 8–12 weeks. Track serum iron and transferrin saturation. Not ferritin alone. If numbers do not rise, ask about inflammation tests. Check CRP or IL-6. You may need to treat inflammation or use IV iron.