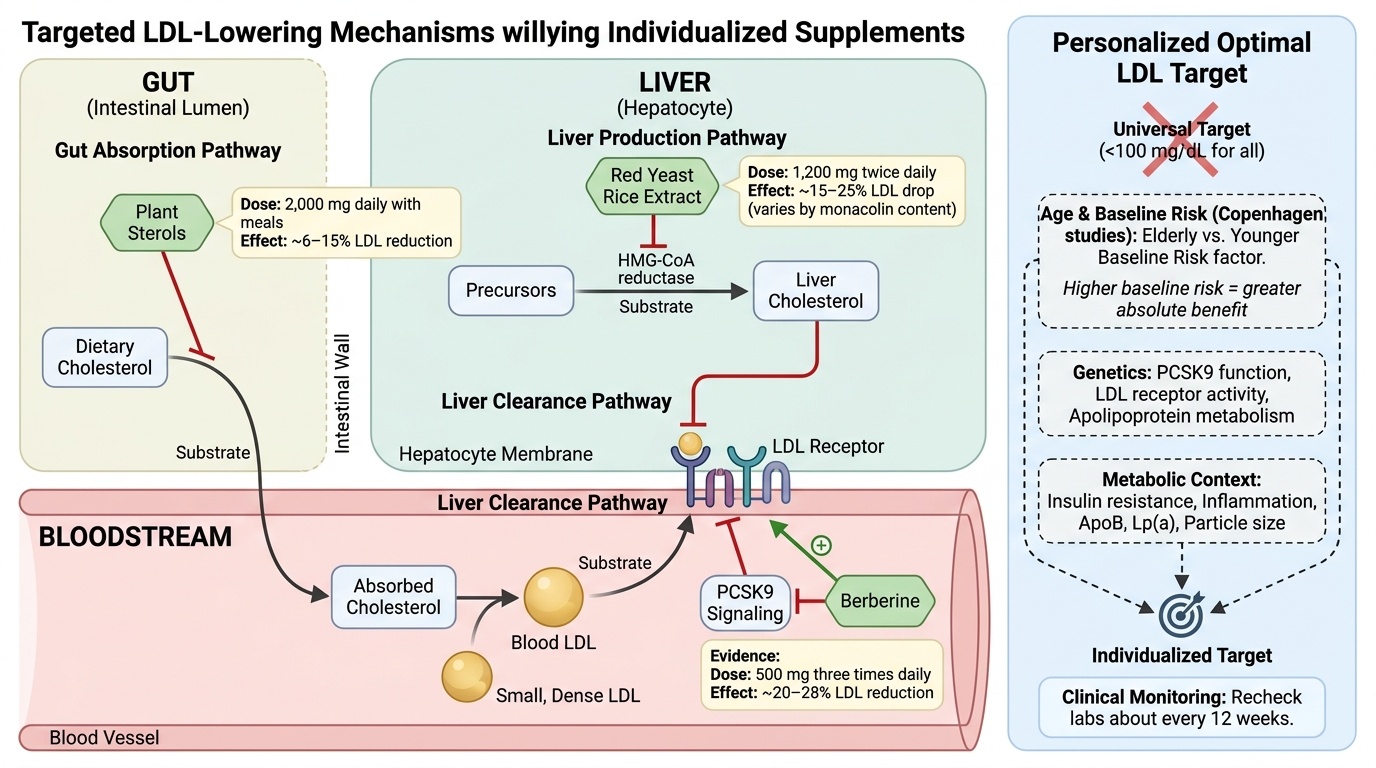
A surprising fact: one LDL goal does not fit everyone. Most people chase one “good” number. But your age and risk change what “good” means.
This means you need a target that fits you. Your best LDL level depends on your full risk picture. That includes family history, ApoB, Lp(a), and inflammation.
You can match supplements to your pattern. Plant sterols: 2,000 mg daily with meals. Red yeast rice extract: 1,200 mg twice daily. Berberine: 500 mg three times daily. Recheck labs about every 12 weeks.