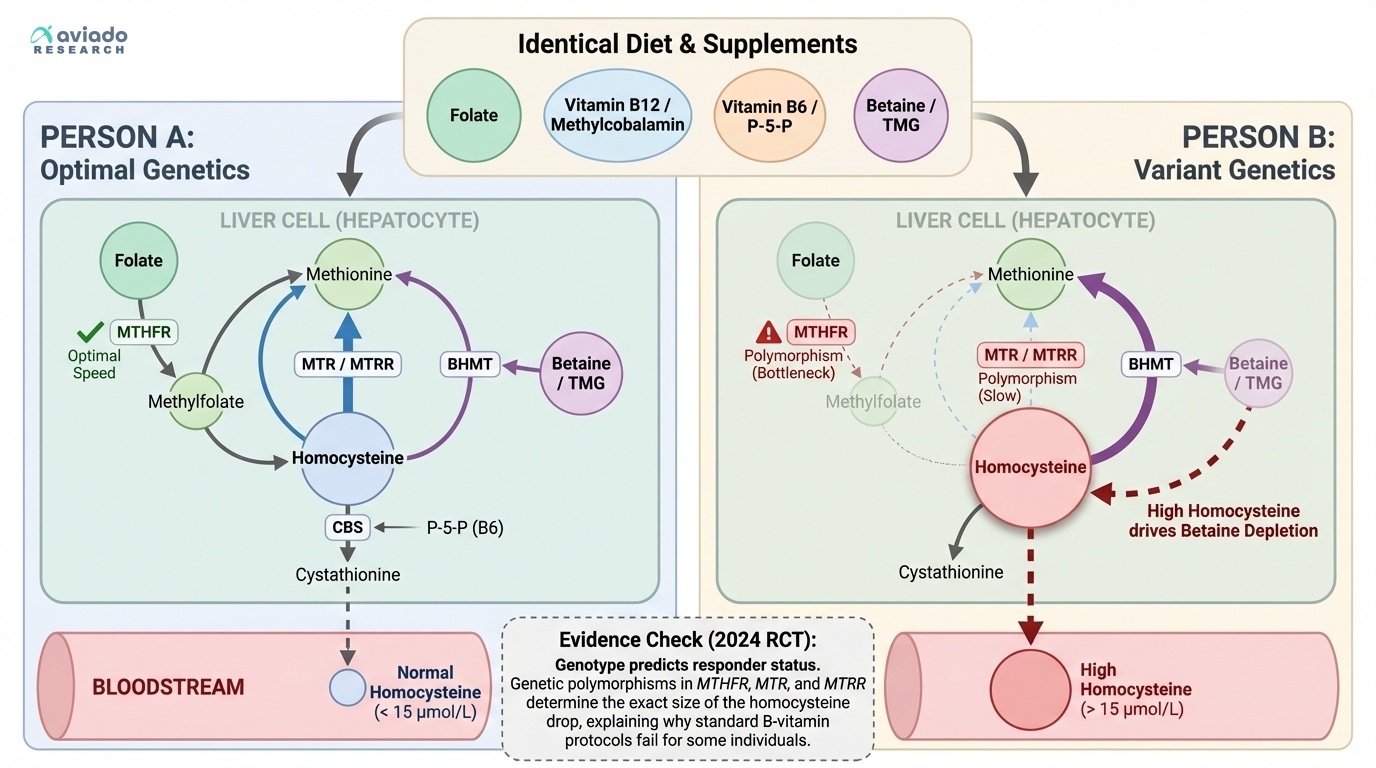
The surprising truth is that homocysteine is not “just diet.” Most people think a high number means you lack B vitamins. Then they take folic acid and hope it drops. But two people can eat the same way and get opposite results.
What this means for you is simple. Your homocysteine is a signal. It shows how well your genes run the methylation cycle. Variants in MTHFR, MTR, and MTRR can change your response. So you may need different forms of B vitamins.
Start with a fasting homocysteine test. If you supplement, use methylfolate 400–800 mcg daily. Add methylcobalamin (B12) 1,000 mcg daily. Add P-5-P (active B6) 25–50 mg daily. If your level stays high, add betaine (TMG) 500–1,000 mg twice daily. Retest in 8–12 weeks.