Unexpectedly, your fish oil may do nothing if your levels stay low. Most people count capsules, not results. Your body may not absorb EPA and DHA well. So you can take it daily and still test low.
This means you should test, not guess. Get an Omega-3 Index blood test first. Then you will know if your dose works. Retest later to confirm the change.
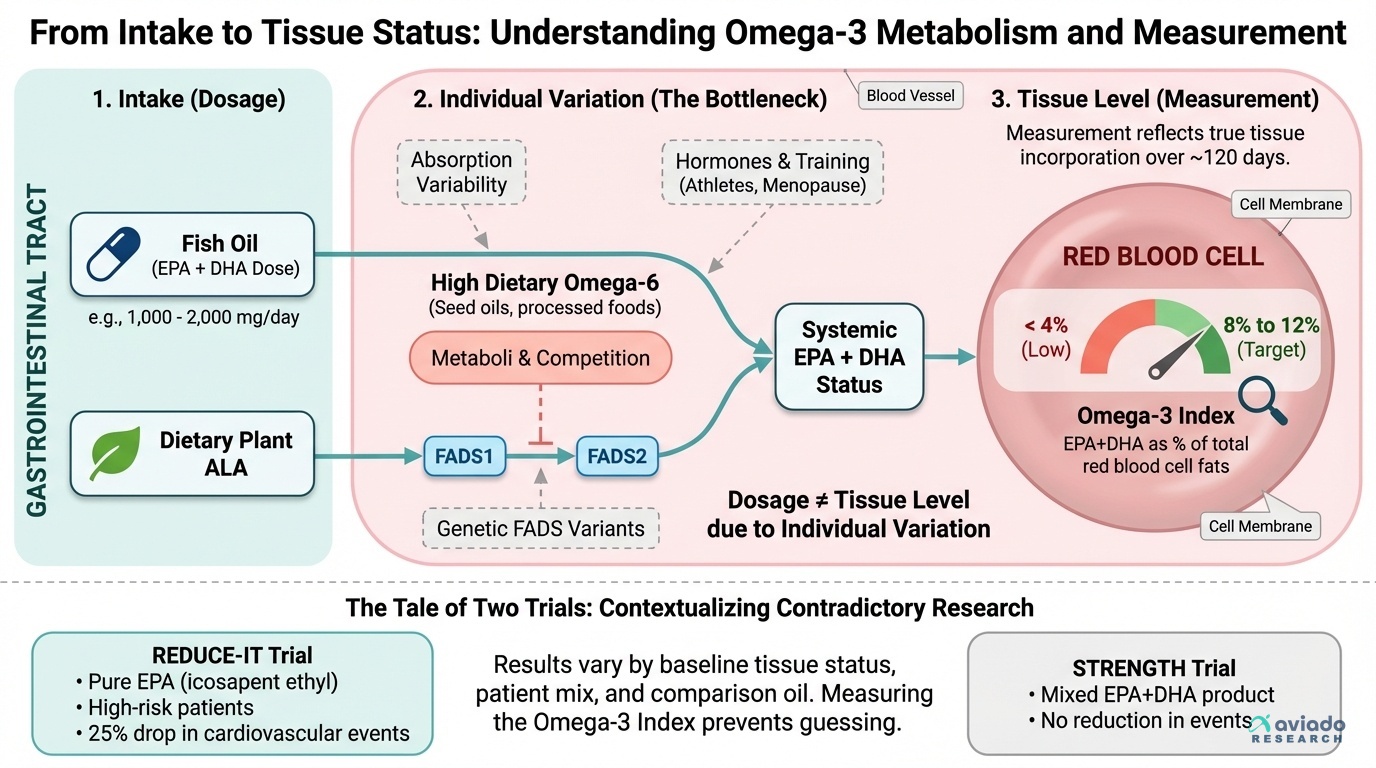
Aim for an Omega-3 Index of 8% to 12%. If you test under 4%, start with 1,000 mg EPA+DHA daily. Many people need 2,000 mg daily total. Try 1,000 mg with breakfast and 1,000 mg with dinner. Retest in 12 weeks and adjust.