For decades, endocrinologists have operated under the free hormone hypothesis: only unbound testosterone can enter cells and create biological effects. This assumption drives the clinical focus on measuring free testosterone rather than just total testosterone. However, recent research is challenging this fundamental principle [1].
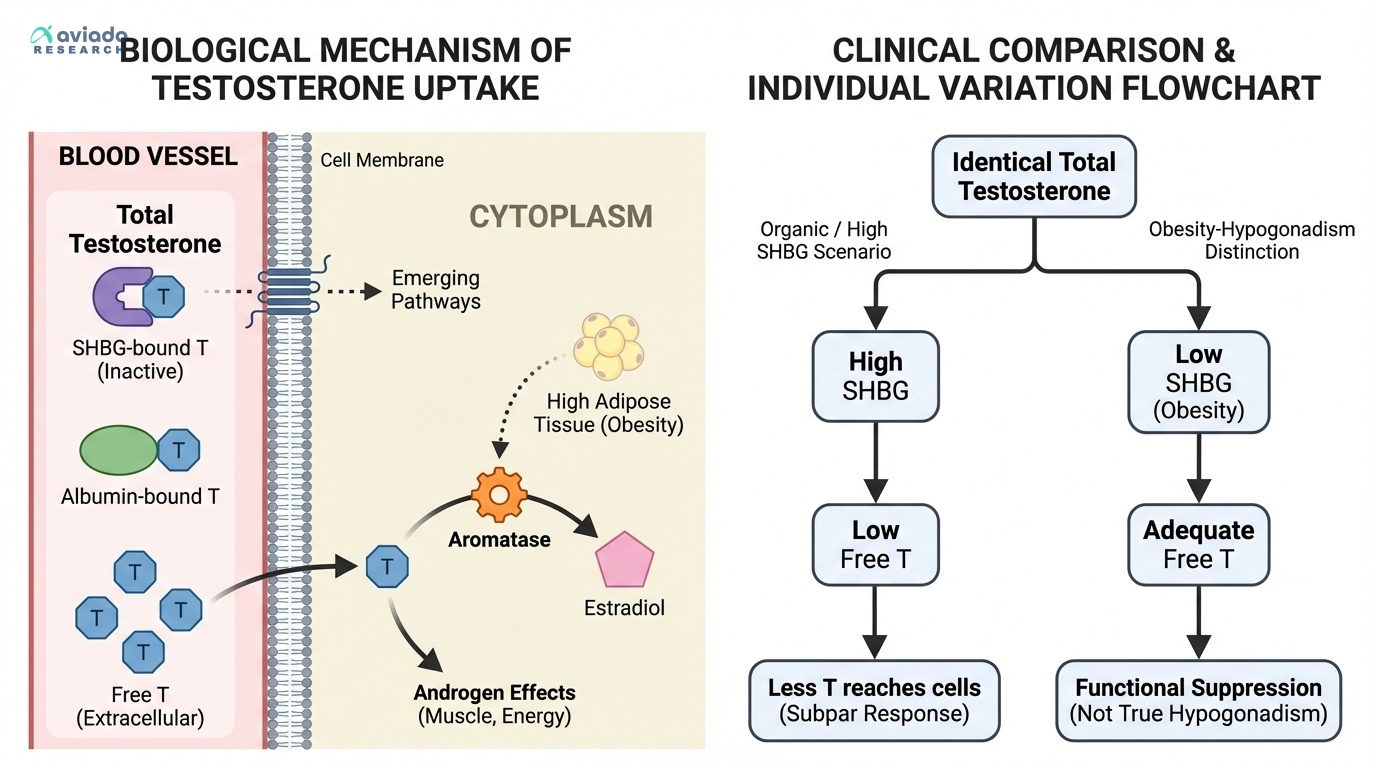
The traditional model suggests that testosterone bound to SHBG is completely inactive, while testosterone bound to albumin can dissociate and become available to tissues. But emerging evidence indicates that SHBG-bound testosterone may have its own biological pathways, and that tissue-specific factors influence hormone uptake in ways that simple blood measurements can't capture.
This reappraisal doesn't invalidate free testosterone testing—it reveals why the same free testosterone level can produce different results in different people. Factors like tissue sensitivity, receptor density, and local enzyme activity create additional layers of variation that explain why some men feel optimal at free testosterone levels that leave others feeling subpar.