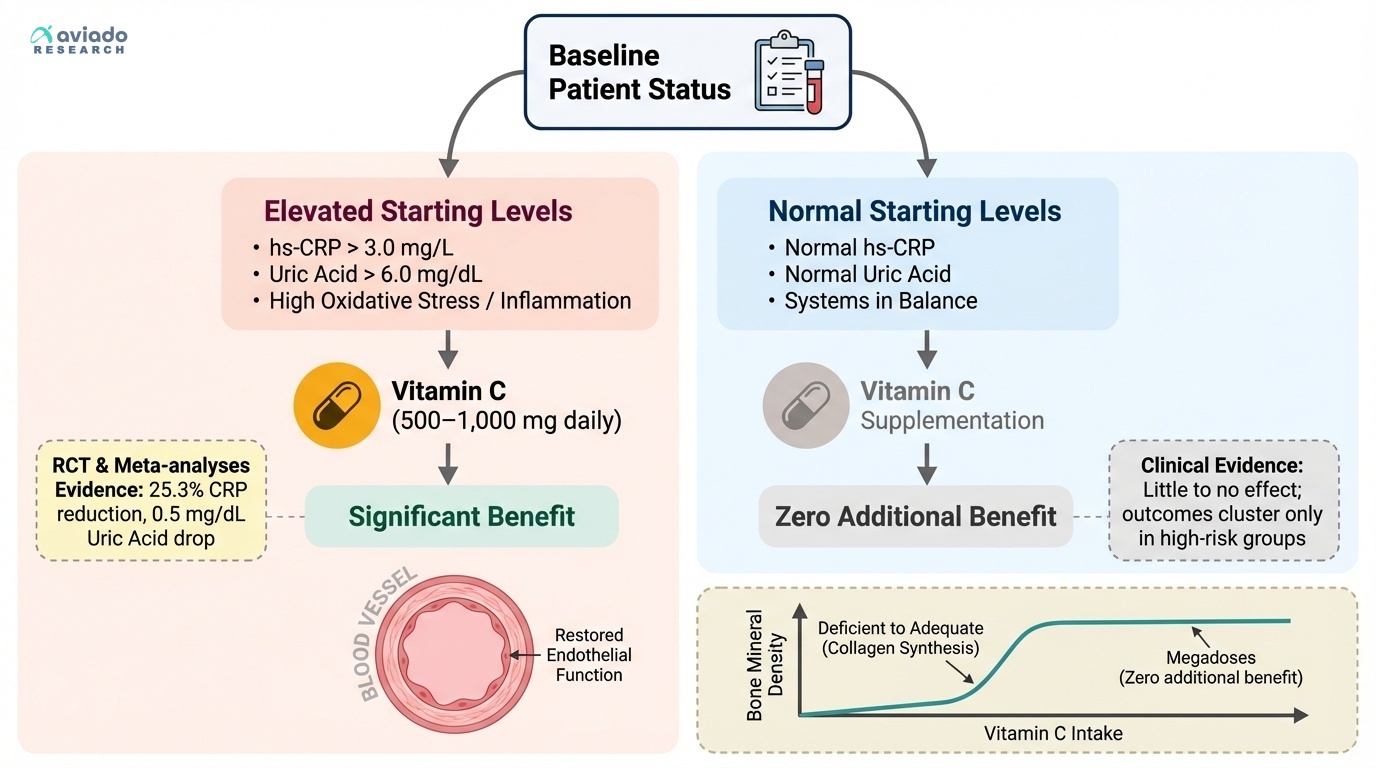
The surprising truth is vitamin C only helps some people. Most people take it daily and expect a boost. But if your labs are normal, nothing changes.
This means you should check your baseline first. Look at hs-CRP, uric acid, and glucose. If they are high, vitamin C may help you. If they are normal, save your money.
If your hs-CRP is over 3 mg/L, try 500–1,000 mg daily. If your uric acid is over 6.0 mg/dL, try 500 mg daily. Retest your labs in 8–12 weeks. Split doses like 500 mg twice daily if needed.