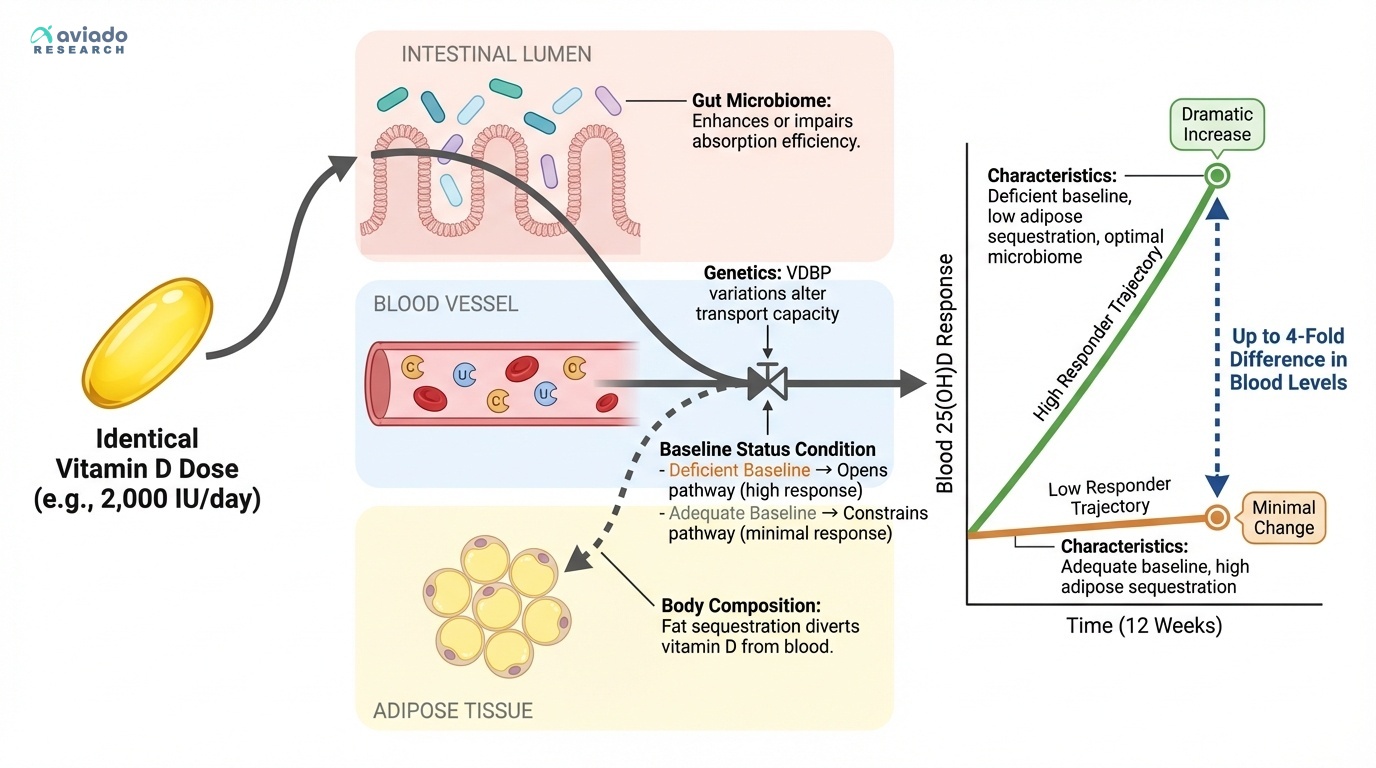
The most important predictor of whether vitamin D supplementation will benefit you isn't your age, weight, or health status — it's where your blood levels start. Research consistently shows that vitamin D's benefits are largely confined to people who begin supplementation from a deficient state [2].
This pattern appears across multiple health outcomes. Studies on immune function, respiratory infections, and even metabolic markers like insulin sensitivity show clear benefits in deficient populations but minimal effects in people with adequate baseline levels. The threshold appears to be around 50 nmol/L (20 ng/mL) — below this level, supplementation often produces measurable benefits; above it, the effects diminish significantly.
The mechanism makes biological sense. Vitamin D functions as a hormone, and like other hormones, there's an optimal range where more isn't necessarily better. Once your tissues have adequate vitamin D availability, additional supplementation doesn't enhance function and may even disrupt normal regulatory mechanisms [3].
This is why the 'take vitamin D and see how you feel' approach fails so often. If you're starting from adequate levels, you won't notice benefits because there aren't any to be had. But if you're starting from deficiency, the same dose might produce dramatic improvements in energy, immune function, or mood.