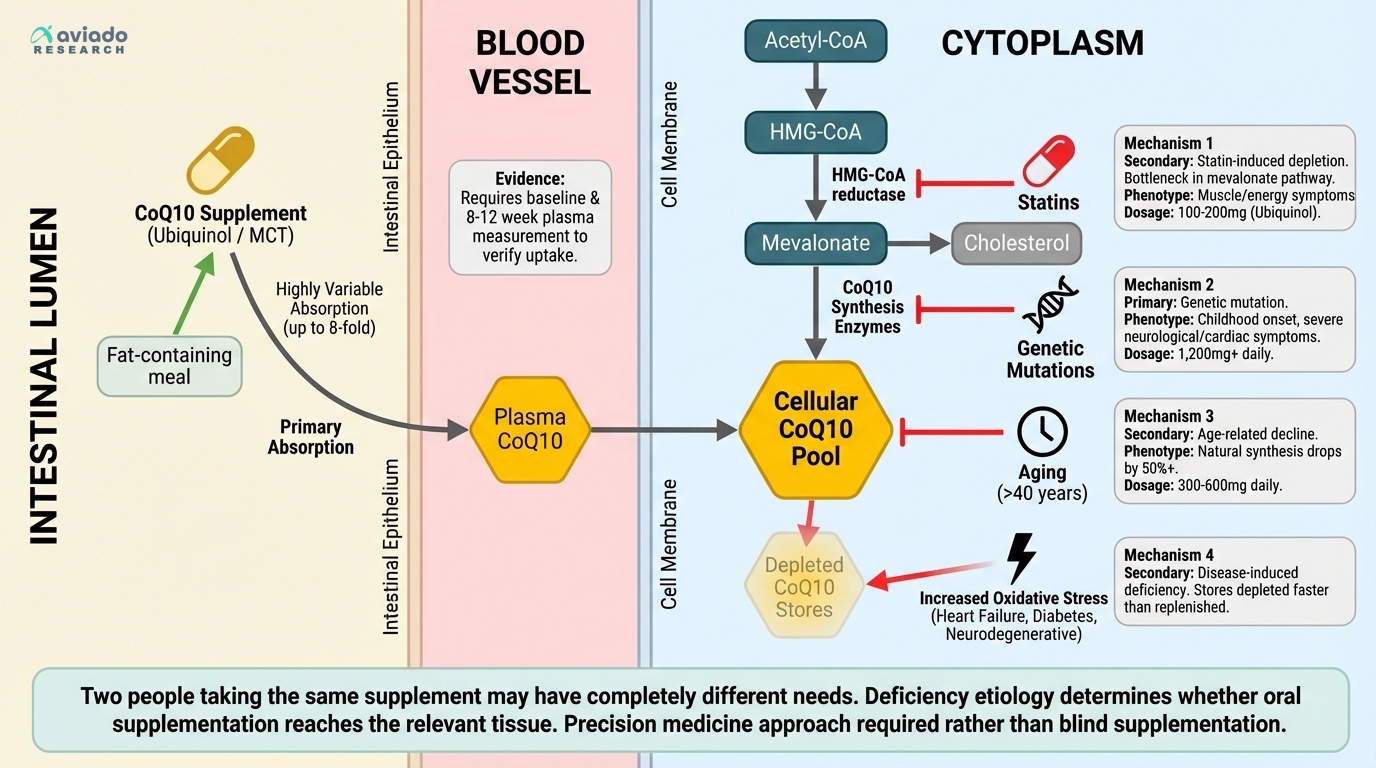
The surprising truth is that CoQ10 deficiency is not one problem. Most people buy a random pill and hope. But low CoQ10 can come from genes, statins, aging, or disease. Each cause acts differently in your body.
This means your best dose depends on your cause. If you take statins, you may lose CoQ10 faster. If you are older, you may make less CoQ10. If you absorb poorly, your blood level may barely move. You can feel no change even with daily pills.
Start with clear steps you can follow. If you take a statin, ask about 100–200 mg ubiquinol daily. If you are over 40, many studies use 300–600 mg daily in better forms. Rare gene disorders may need up to 1,200 mg daily. Take CoQ10 with a fat meal for better uptake.